


 Sign Out
Sign Out



Most HPV infections clear without sequelae but some progress to HPV-related diseases including cervical cancers and their precursors (Cervical Intraepithelial Neoplasia or CIN grades 1, 2, and 3), anal, vulvar, vaginal, and penile cancers and their precursors (Anal Intraepithelial Neoplasia or AIN, Vulvar Intraepithelial Neoplasia or VIN, Vaginal Intraepithelial Neoplasia or VaIN and Penile Intraepithelial Neoplasia or PIN), genital warts, and lesions in the aerodigestive tract including oropharyngeal cancers and recurrent respiratory papillomatosis.
Worldwide, over 530,000 cases of cervical cancer are diagnosed annually. Cervical cancer prevention focuses on repeat screening (e.g., Papanicolaou's [Pap] testing and/or Human Papillomavirus [HPV] testing) and early intervention. This strategy has reduced cancer rates by approximately 75% in the developed world but has shifted the burden from managing cervical cancer to monitoring and treating a large number of premalignant lesions.
GARDASIL 9 is a recombinant vaccine with L1 proteins resembling 9 HPV types. Because the L1 proteins contain no viral DNA, they cannot infect cells or reproduce. GARDASIL 9 contains the 4 HPV types (6, 11, 16, and 18) that are in GARDASIL plus an additional 5 HPV types (31, 33, 45, 52, and 58) adsorbed on amorphous aluminum hydroxyphosphate adjuvant (AAHS). The attribution of the 9 HPV types in GARDASIL 9 to HPV-related disease worldwide is presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinical Studies: GARDASIL 9 includes the same four HPV types contained in GARDASIL (HPV 6, 11, 16, 18) and five additional HPV types (31, 33, 45, 52, and 58).
Efficacy Data for GARDASIL: GARDASIL was first licensed in 2006. Efficacy was assessed in 6 AAHS-controlled, double-blind, randomized Phase II and III clinical studies evaluating 28,413 individuals (20,541 girls and women 16 through 26 years of age, 4,055 boys and men 16 through 26 years of age, 3,817 women 24 through 45 years of age). GARDASIL was efficacious in reducing the incidence of CIN (any grade including CIN 2/3); AIS; genital warts; VIN 2/3; and VaIN 2/3 related to vaccine HPV types 6, 11, 16, or 18 in those girls and women who were PCR negative and seronegative at baseline (Table 2). In addition, girls and women who were already infected with 1 or more vaccine-related HPV types prior to vaccination were protected from precancerous cervical lesions and external genital lesions caused by the other vaccine HPV types. Individuals who had prior infection that had been resolved before vaccination (PCR negative and seropositive at baseline) were protected from reinfection or recurrence of infection leading to clinical disease with the same HPV type. GARDASIL was efficacious in reducing the incidence of genital warts related to vaccine HPV types 6 and 11 in boys and men who were PCR negative and seronegative at baseline. Efficacy against penile/perineal/perianal intraepithelial neoplasia (PIN) grades 1/2/3 or penile/perineal/perianal cancer was not demonstrated as the number of cases was too limited to reach statistical significance (Table 2). GARDASIL was efficacious in reducing the incidence of anal intraepithelial neoplasia (AIN) grades 1 (both condyloma and non-acuminate), 2, and 3 related to vaccine HPV types 6, 11, 16, and 18 in boys and men who were PCR negative and seronegative at baseline (Table 2). (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA minimum anti-HPV level that provides protection against HPV infection and disease has not been defined. Also, immune responses to vaccines are typically lower in older individuals compared to younger individuals. Therefore, to confirm the utility of GARDASIL to prevent cervical, vulvar, and vaginal cancers and related diseases caused by the types targeted by the vaccine in individuals up to and including age 45 years, an efficacy study was conducted.
GARDASIL was highly efficacious in reducing the incidence of persistent infection; CIN (any grade); and external genital lesions (EGL) caused by HPV types 6, 11, 16, and 18. GARDASIL was also highly efficacious in reducing the incidence of a HPV 16/18-related Pap Test diagnosis of ASC-US (Atypical Squamous Cells of Undetermined Significance) positive for high-risk HPV. The primary analyses of efficacy, with respect to HPV types 6, 11, 16, and 18, were conducted in the per-protocol efficacy (PPE) population. Efficacy was measured starting after the Month 7 visit.
On the basis of these efficacy findings, the efficacy of GARDASIL with respect to prevention of cervical, vulvar, and vaginal cancers and related diseases in individuals up to and including age 45 years can be inferred. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEffectiveness of GARDASIL in men 27 through 45 years of age is inferred from efficacy data in women 24 through 45 years of age as described previously and supported by immunogenicity data from a clinical trial in which 150 men, 27 through 45 years of age received a 3-dose regimen of GARDASIL (0, 2, 6 months). A cross-study analysis of per-protocol immunogenicity populations compared Month 7 anti-HPV 6, 11, 16, and 18 GMTs of these 27- through 45-year-old men to those of 16- through 26-year-old boys and men in whom efficacy of GARDASIL had been established (see Table 6). GMT ratios (27- through 45-year-old men/16- through 26-year-old boys and men) for HPV 6, 11, 16, and 18 were 0.82 (95%CI: 0.65, 1.03), 0.79 (95%CI: 0.66, 0.93), 0.91 (95%CI: 0.72, 1.13), and 0.74 (95%CI: 0.59, 0.92), respectively.
Long-term follow-up studies: A subset of subjects who received 3 doses were followed up for 10 to 14 years after GARDASIL vaccination for safety, immunogenicity and protection against clinical diseases related to HPV types 6/11/16/18.
Persistence of antibody response was observed for 10 years in adolescents who were 9 through 15 years of age at time of vaccination; 14 years in girls and women, 16 through 23 years of age at time of vaccination; 9.5 years in boys and men, 16 through 26 years of age at time of vaccination, and 9.5 years in women, 24 through 45 years of age at time of vaccination.
Clinical protection was observed in all subjects in the PPE population: no cases of HPV diseases were observed after a follow-up of approximately 10.7 years (median duration of follow-up of 10.0 years) in girls who were 9 through 15 years of age at time of vaccination; 10.6 years (median duration of follow-up of 9.9 years) in boys, 9 through 15 years of age at time of vaccination; 14 years (median duration of follow-up of 11.9 years) in girls and women, 16 through 23 years of age at time of vaccination; 11.5 years (median duration of follow-up of 9.5 years) in boys and men, 16 through 26 years of age at time of vaccination, and 10.1 years (median duration of follow-up of 8.7 years) in women, 24 through 45 years of age at time of vaccination.
Persistence of antibody response to GARDASIL was also assessed in a clinical trial using a 2-dose regimen. One month after the last dose, antibody responses to the 4 HPV types were non-inferior among girls 9 through 13 years of age who received 2 doses of GARDASIL 6 months apart compared with girls and women 16 through 26 years of age who received 3 doses of the vaccine within 6 months. In post hoc analyses at 3 and 10 years of follow-up, non-inferiority criteria were also met for all 4 HPV types.
Clinical Trials for GARDASIL 9: Efficacy and/or immunogenicity of the 3-dose regimen of GARDASIL 9 were assessed in nine clinical studies. Clinical studies evaluating the efficacy of GARDASIL 9 against placebo were not acceptable because HPV vaccination represents the standard of care for protection against HPV infection and disease in many countries. Therefore, the pivotal clinical study (Protocol 001) evaluated the efficacy of GARDASIL 9 to prevent HPV-related cervical, vulvar, and vaginal disease using GARDASIL as a comparator.
Efficacy against HPV Types 6, 11, 16, and 18 was primarily assessed using a bridging strategy that demonstrates comparable immunogenicity (as measured by Geometric Mean Titers [GMT]) of GARDASIL 9 compared with GARDASIL (Protocols 001, 009 and 020).
The analysis of efficacy for GARDASIL 9 was evaluated in the PPE population of 16- through 26-year-old girls and women, who were naïve to the relevant HPV type(s) prior to dose one and through 1 month Postdose 3 (Month 7). Overall, approximately 52% of subjects were negative to all vaccine HPV types by both PCR and serology at Day 1.
The primary analysis of efficacy against HPV Types 31, 33, 45, 52, and 58 is based on a combined endpoint of Cervical Intraepithelial Neoplasia (CIN) 2, CIN 3, Adenocarcinoma in situ (AIS), invasive cervical carcinoma, Vulvar Intraepithelial Neoplasia (VIN) 2/3, Vaginal Intraepithelial Neoplasia (VaIN) 2/3, vulvar cancer, or vaginal cancer. Other endpoints evaluated include cervical, vulvar, and vaginal disease of any grade; persistent infection; cytological abnormalities and invasive procedures. For all endpoints, the efficacy against the HPV Types in GARDASIL 9 (31, 33, 45, 52, and 58) was evaluated compared to GARDASIL.
The efficacy is further extended to 9- through 15-year-old adolescents and to 16- through 26-year-old boys and men, for all endpoints studied, using immunological bridging. The immunogenicity bridging analyses were performed in the per-protocol immunogenicity (PPI) population consisting of individuals who received all 3 vaccinations within pre-defined day ranges, met pre-defined criteria for the interval between the Month 6 and Month 7 visit, did not have major deviations from the study protocol, and were naïve [PCR negative (in girls and women 16 through 26 years of age; Protocol 001 and 002) and seronegative (Protocols 001, 002, 003, 005, 007 and 009)] to the relevant HPV type(s) prior to dose 1 and through Month 7.
Protocol 001 evaluated efficacy and immunogenicity of GARDASIL 9 to prevent infection and disease caused by HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58 in 16- through 26-year-old girls and women (N = 14,204: 7,099 receiving GARDASIL 9; 7,105 receiving GARDASIL). Two immunological bridging studies evaluated HPV types 6, 11, 16 and 18 (Protocols 002 and 009) and HPV types 31, 33, 45, 52, and 58 (Protocol 002). Protocol 002 evaluated immunogenicity of GARDASIL 9 in girls and boys 9 through 15 years of age and women 16 through 26 years of age (N=3,066: 1,932 girls; 666 boys; and 468 women receiving GARDASIL 9). Protocol 009 evaluated immunogenicity in girls 9 through 15 years of age (N=600; 300 receiving GARDASIL 9 and 300 receiving GARDASIL). Protocol 003 evaluated immunogenicity of GARDASIL 9 in boys and men 16 through 26 years of age and in girls and women 16 through 26 years of age (N=2,515: 1,103 Heterosexual Men [HM]; 313 Men Who Have Sex with Men [MSM]; and 1,099 women receiving GARDASIL 9). Protocol 006 evaluated administration of GARDASIL 9 to girls and women 12 through 26 years of age previously vaccinated with GARDASIL (N=921; 615 receiving GARDASIL 9 and 306 receiving placebo). Protocols 005 and 007 evaluated GARDASIL 9 concomitantly administered with vaccines recommended routinely in girls and boys 11 through 15 years of age (N=2,295). Together, these seven studies evaluated 15,875 individuals who received GARDASIL 9 (9,152 girls and women 16 through 26 years of age at enrollment with a mean age of 21.7 years; 3,498 girls 9 through 15 years of age at enrollment with a mean age of 12.0 years; 1,416 boys and men 16 through 26 years of age at enrollment with a mean age of 21.1 years; and 1,809 boys 9 through 15 years of age at enrollment with a mean age of 12.1 years.
Two additional immunological bridging studies were conducted. Protocol 020 evaluated immunogenicity of GARDASIL 9 compared to GARDASIL in boys and men 16 through 26 years of age (N=500: 249 receiving GARDASIL 9 and 251 receiving GARDASIL). Protocol 004 evaluated immunogenicity of GARDASIL 9 in girls and women 16 through 26 years of age compared to women 27 through 45 years of age (N=1,210: 640 women 27 through 45 years and 570 girls and women 16 through 26 years).
One clinical trial (Protocol 010) assessed the 2-dose regimen of GARDASIL 9. Protocol 010 evaluated the immunogenicity of 2 doses of GARDASIL 9 in girls and boys 9 through 14 years of age and 3 doses of GARDASIL 9 in girls 9 through 14 years of age and girls and women 16 through 26 years of age; (N = 1,516; 751 girls; 451 boys and 314 women). The mean age for the girls and boys 9 through 14 years of age was 11.5 years; the mean age for the girls and women 16 through 26 years of age was 21.0 years.
The totality of results from the clinical studies support that GARDASIL 9 was efficacious against HPV disease and persistent infection caused by HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. Therefore the efficacy for cervical, vulvar, vaginal, and anal diseases, genital warts and persistent infection that was demonstrated in the original clinical studies for GARDASIL can be extended to GARDASIL 9. In clinical studies, protective efficacy has been shown to last up to 5.6 years postdose 3 in duration for GARDASIL 9.
The decision to vaccinate an individual should take into account the risk for previous HPV exposure and potential benefit from vaccination.
Comparison of Immune Responses Between GARDASIL 9 and GARDASIL for HPV Types 6, 11, 16, and 18 in the Clinical Studies for GARDASIL 9: Studies Supporting the Efficacy of GARDASIL 9 Against HPV Types 6, 11, 16, 18: Because of the high efficacy of GARDASIL, there is no known immune correlate of protection. The minimal anti-HPV response associated with protection against HPV 6-, 11-, 16-, and 18-related infection and disease has not been established. In addition, the existence of HPV Types 6, 11, 16, and 18 antigens in both the formulations for GARDASIL 9 and the active comparator vaccine (GARDASIL) should result in no or few infection and disease endpoints associated with these HPV types. A low number of efficacy endpoints in both vaccination groups preclude a direct measurement of efficacy using disease endpoints associated with these HPV types.
GARDASIL 9 efficacy against HPV 6-, 11-, 16-, and 18-related infection and disease was inferred from comparative studies to the quadrivalent HPV (Types 6, 11, 16, 18) vaccine, GARDASIL, in which GARDASIL 9 elicited immune responses as measured by GMT. These studies were designed to evaluate immunologic non-inferiority of GARDASIL 9 to GARDASIL. Therefore, the efficacy findings from the pivotal clinical studies for GARDASIL against HPV Type 6-, 11-, 16-, and 18-related disease were extended to GARDASIL 9 by demonstrating that the immune responses elicited by GARDASIL 9 were non-inferior to the immune responses elicited by GARDASIL.
Comparison of GARDASIL 9 with GARDASIL immunogenicity with respect to HPV types 6, 11, 16, and 18 were conducted in a population of 16- through 26-year-old women from Protocol 001, 9- through 15-year-old girls from Protocol 009 and 16- through 26-year-old boys from Protocol 020. The primary analyses were conducted in the per-protocol immunogenicity population which included subjects who received all 3 vaccinations within pre-defined day ranges, met pre-defined criteria for the interval between the Month 6 and Month 7 visit, did not have major deviations from the study protocol, and were naïve [PCR negative (in girls and women 16 through 26 years of age; Protocol 001) and seronegative (Protocols 001, 009 and 020) prior to dose one] to the relevant HPV type(s) and who remained PCR-negative (in girls and women 16 through 26 years of age; Protocol 001) to the relevant HPV type(s) through Month 7.
A statistical analysis of non-inferiority was performed based on Month 7 cLIA anti-HPV 6, anti-HPV 11, anti-HPV 16, and anti-HPV 18 GMTs between individuals administered GARDASIL 9 and individuals administered GARDASIL. Immune responses, measured by GMT, for GARDASIL 9 were non-inferior to immune responses for GARDASIL (Table 4). Therefore, efficacy for GARDASIL 9 against persistent infection and disease related to HPV Types 6, 11, 16, or 18 can be inferred to be comparable to that of GARDASIL. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageProphylactic Efficacy of GARDASIL 9 for HPV Types 31, 33, 45, 52, and 58 in Girls and Women 16 through 26 Years of Age: Studies Supporting Efficacy of GARDASIL 9 Against HPV Types 31, 33, 45, 52, and 58: The efficacy of GARDASIL 9 in 16- through 26- year-old women was assessed in an active comparator-controlled, double-blind, randomized clinical study (Protocol 001) that included a total of 14,204 women (GARDASIL 9 = 7,099; GARDASIL = 7,105), who were enrolled and vaccinated without pre-screening for the presence of HPV infection. Subjects were followed up to 67 months postdose 3, with a median duration of 43 months.
The primary efficacy is based on evaluation of a composite clinical endpoint of HPV 31-, 33-, 45-, 52-, and 58- related cervical cancer, vulvar cancer, vaginal cancer, CIN 2/3 or AIS, VIN 2/3, and VaIN 2/3. The efficacy is further supported by evaluation of HPV 31-, 33-, 45-, 52-, and 58-related cervical, vulvar, and vaginal disease of any grade, and persistent infection. In addition, the study also evaluated the impact of GARDASIL 9 on the rates of HPV 31-, 33-, 45-, 52-, and 58- related abnormal Pap tests, cervical and external genital procedures (i.e., biopsies) and cervical definitive therapy procedures.
Efficacy was evaluated in the PPE population of 16- through 26-year-old women, who were naïve to the relevant HPV type(s) prior to dose one and through Month 7. Efficacy was measured starting after the Month 7 visit. GARDASIL 9 was efficacious in preventing HPV 31-, 33-, 45-, 52-, and 58- related persistent infection and disease (Table 5). GARDASIL 9 also reduced the incidence of HPV 31-, 33-, 45-, 52-, and 58- related Pap test abnormalities, cervical procedures (i.e., biopsies), and cervical definitive therapy procedures (including loop electrosurgical excision procedure [LEEP] or conization). See Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional Efficacy Evaluation of GARDASIL 9 Against HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58: Since the efficacy of GARDASIL 9 could not be evaluated against placebo, the following exploratory analyses were conducted.
Efficacy Evaluation of GARDASIL 9 Against Cervical High Grade Diseases Caused by HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 in the PPE: The efficacy of GARDASIL 9 against CIN 2 and worse related to HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 compared to GARDASIL was 94.4% (95% CI 78.8; 99.0) with 2/5,952 versus 36/5,947 cases. The efficacy of GARDASIL 9 against CIN 3 related to HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 compared to GARDASIL was 100% (95% CI 46.3; 100.0) with 0/5,952 versus 8/5,947 cases. These results reflect efficacy of GARDASIL 9 versus GARDASIL against disease caused by HPV types 31, 33, 45, 52, and 58 since both vaccines are efficacious in preventing disease related to HPV types 6, 11, 16, 18.
Impact of GARDASIL 9 Against Cervical Biopsy and Definite Therapy Related to HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 in the PPE: The efficacy of GARDASIL 9 against cervical biopsy related to HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 compared to GARDASIL was 95.9% (95% CI 92.7; 97.9) with 11/6,016 versus 262/6,018 cases. The efficacy of GARDASIL 9 against cervical definitive therapy (including loop electrosurgical excision procedure [LEEP] or conization) related to HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 compared to GARDASIL was 90.7% (95% CI 76.3; 97.0) with 4/6,016 versus 43/6,018 cases. These results reflect efficacy of GARDASIL 9 versus GARDASIL against procedures associated with HPV types 31, 33, 45, 52, and 58 since both vaccines are efficacious in preventing disease related to HPV types 6, 11, 16, 18.
Long-term effectiveness studies: A subset of subjects who received 3 doses is being followed up for 10 to 14 years after GARDASIL 9 vaccination for safety, immunogenicity, and effectiveness against clinical diseases related to the HPV types 6/11/16/18/31/33/45/52/58.
Clinical protection has been observed in all subjects in the long-term extension of Protocol 001 registry study in the PPE population. No cases of high-grade CIN were observed through 9.5 years postdose 3 (median duration of follow-up of 6.3 years) in girls and women who were 16 through 26 years of age at time of vaccination.
In the long-term extension of Protocol 002, no cases of high-grade intraepithelial neoplasia or genital warts were observed through 11 years postdose 3 (median duration of follow-up of 10.0 years) in girls and through 10.6 years postdose 3 (median duration of follow-up of 9.9 years) in boys who were 9 through 15 years of age at time of vaccination with GARDASIL 9. In girls and boys, incidence rates of 6-month persistent infections related to vaccine HPV types observed during the study were 52.4 and 54.6 per 10,000 person-years, respectively, and within ranges of incidence rates expected in vaccinated cohorts of similar age (based on results from previous efficacy studies of GARDASIL 9 and GARDASIL vaccine).
Immunogenicity of GARDASIL 9: Assays to Measure Immune Response: The minimum anti-HPV titer that confers protective efficacy has not been determined.
Because there were few disease cases in individuals naïve (PCR negative and seronegative) to vaccine HPV types at baseline in the group that received GARDASIL 9 it has not been possible to establish minimum antibody levels that protect against clinical disease caused by vaccine HPV types.
Type-specific immunoassays with type-specific standards were used to assess immunogenicity to each vaccine HPV type. These assays measured antibodies against neutralizing epitopes for each HPV type. The scales for these assays are unique to each HPV type; thus, comparisons across types and to other assays are not appropriate.
Immune Response to GARDASIL 9 at Month 7 In Clinical Studies: The primary immunogenicity analyses were conducted in a per-protocol immunogenicity (PPI) population. This population consisted of individuals who received all 3 vaccinations within pre-defined day ranges, met pre-defined criteria for the interval between the Month 6 and Month 7 visit, did not have major deviations from the study protocol, and were naïve [PCR negative (in girls and women 16 through 26 years of age) and seronegative prior to dose one] to the relevant HPV type(s) and who remained PCR-negative (in girls and women 16 through 26 years of age) to the relevant HPV type(s) through Month 7.
Immunogenicity was measured by (1) the percentage of individuals who were seropositive for antibodies against the relevant vaccine HPV type, and (2) the Geometric Mean Titer (GMT).
GARDASIL 9 induced robust anti-HPV 6, anti-HPV 11, anti-HPV 16, anti-HPV 18, anti-HPV 31, anti-HPV 33, anti-HPV 45, anti-HPV 52, and anti-HPV 58 responses measured at Month 7 (Table 6). In clinical studies 99.2% to 100% who received GARDASIL 9 became seropositive for antibodies against all 9 vaccine types by Month 7 across all groups tested. GMTs were higher in girls and boys than in women 16 through 26 years of age, and higher in boys than in girls and women. As expected for women 27 through 45 years of age (Protocol 004), the observed GMTs were lower than those seen in girls and women 16 through 26 years of age. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTable 6 displays the Month 7 immunogenicity data for girls and women and boys. Anti-HPV responses at Month 7 among 9- through 15-year-old girls were comparable to anti-HPV responses in 16- through 26-year-old women in the combined database of immunogenicity studies for GARDASIL 9. Anti-HPV responses at Month 7 among 9- through 15-year-old boys were comparable to anti-HPV responses in both 16- through 26-year-women and 9- through 15-year-old girls.
On the basis of this immunogenicity bridging, the efficacy of GARDASIL 9 in 9- through 15-year-old girls and boys is inferred.
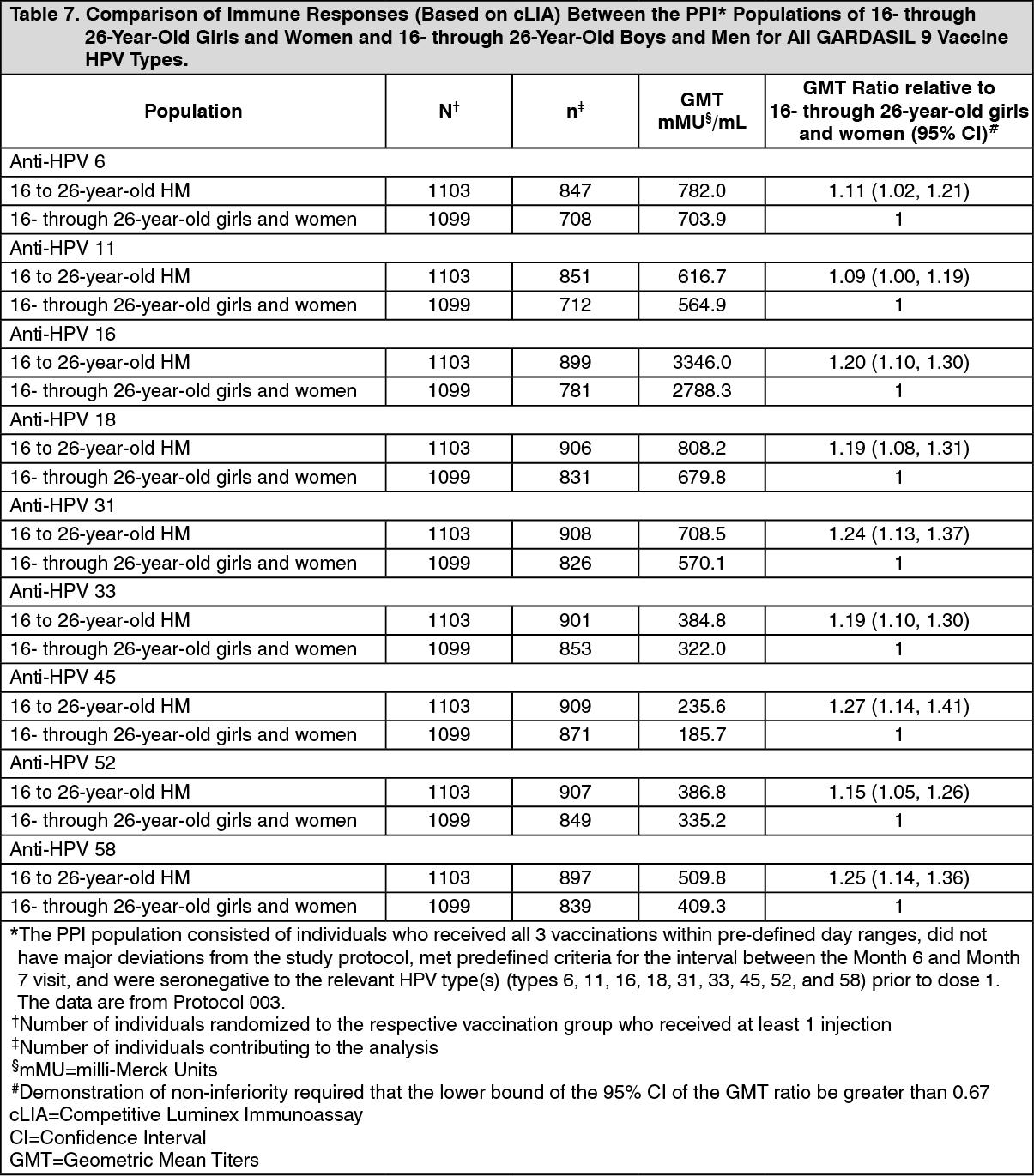
Study Supporting the Effectiveness of GARDASIL 9 against Vaccine HPV Types in 16- through 26-Year-Old Boys and Men: Effectiveness of GARDASIL 9 against persistent infection and disease related to vaccine HPV types in 16- through 26-year-old boys and men was inferred from non-inferiority comparison in Protocol 003 of GMTs following vaccination with GARDASIL 9 among 16- to 26-year-old boys and men with those among 16- through 26-year-old girls and women. The primary analyses were conducted in the per-protocol population, which included subjects who received all 3 vaccinations within pre-defined day ranges, met pre-defined criteria for the interval between the Month 6 and Month 7 visit, did not have major deviations from the study protocol, and were seronegative to the relevant HPV type(s) prior to dose 1. Anti-HPV GMTs at Month 7 among 16- through 26-year-old boys and men (HM) were non-inferior to anti-HPV GMTs among 16- through 26-year-old girls and women (Table 7). Anti-HPV GMTs at Month 7 among 16- through 26-year-old MSM (HIV-negative) were lower than in 16- through 26-year-old HM. The GMT fold difference in 16- through 26-year-old MSM relative to the HM was 0.6 to 0.8; anti-HPV GMTs for the MSM subjects ranged between 157.5 and 2294.0 mMU/mL. The fold differences observed with GARDASIL 9 for MSM compared to HM were generally similar to those previously observed with GARDASIL. In Protocol 003, 99.6% to 100% in the HM population and 99.4 to 100% in the MSM population who received GARDASIL 9 became seropositive for antibodies against all 9 vaccine types by Month 7. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOn the basis of this immunogenicity bridging, the efficacy of GARDASIL 9 in 16- through 26-year-old boys and men is inferred.
Women 27 Years of Age and Older: Effectiveness of GARDASIL 9 against persistent infection and disease related to vaccine HPV types in 27- through 45-year-old women was inferred based on non-inferiority of GMTs following vaccination with GARDASIL 9 in 27- through 45-year-old women compared to 16- through 26-year-old girls and women and demonstration of efficacy of GARDASIL in girls and women 16 through 45 years of age. In Protocol 004, GARDASIL 9 elicited seroconversion rates for all nine vaccine HPV types greater than 99% in girls and women 16 through 45 years of age. Anti-HPV antibody GMTs at Month 7 among women 27 through 45 years of age were non-inferior to anti-HPV antibody GMTs among girls and women 16 through 26 years of age for HPV 16, 18, 31, 33, 45, 52, and 58, with GMT ratios between 0.66 and 0.73. In a post hoc analysis for HPV 6 and 11, non-inferiority criteria were also met, with GMT ratios of 0.81 and 0.76, respectively. These results support the efficacy of GARDASIL 9 in women 27 through 45 years of age. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMen 27 Years of Age and Older: GARDASIL 9 has not been studied in men 27 years of age and older. In men 27 years of age and older, efficacy of GARDASIL 9 is inferred based on (1) high efficacy of GARDASIL in girls and women 16 through 45 years of age and (2) comparable efficacy and immunogenicity of GARDASIL and GARDASIL 9 in individuals less than 27 years of age and (3) robust immunogenicity of GARDASIL in boys and men 16 through 45 years of age.
Immune Responses to GARDASIL 9 Using a 2-dose Schedule in Individuals 9- through 14 Years of Age: Protocol 010 measured HPV antibody responses to the 9 HPV types after GARDASIL 9 vaccination in the following cohorts: girls and boys 9 through 14 years of age receiving 2 doses at a 6-month or 12-month interval (+/- 1 month); girls 9 through 14 years of age receiving 3 doses (at 0, 2, 6 months); and women 16 through 26 years of age receiving 3 doses (at 0, 2, 6 months).
GMTs were non-inferior in girls and boys who received 2 doses of GARDASIL 9 (at either 0, 6 months or 0, 12 months) to GMTs in 16- through 26-year-old girls and women who received 3 doses of GARDASIL 9 (at 0, 2, 6 months) for each of the 9 vaccine HPV types. On the basis of this immunogenicity bridging, the efficacy of a 2-dose regimen of GARDASIL 9 in 9- through 14-year-old girls and boys is inferred. One month following the last dose of the assigned regimen, between 97.9% and 100% of subjects across all groups became seropositive for antibodies against the 9 vaccine HPV types (Table 9).
In the same study, in girls and boys 9 through 14 years of age, GMTs at one month after the last vaccine dose were numerically lower for some vaccine types after a 2-dose schedule than in girls 9 through 14 years of age after a 3-dose schedule (HPV types 18, 31, 45, and 52 after 0, 6 months and HPV type 45 after 0, 12 months; Table 9). The clinical relevance of these findings is unknown.
Persistence of antibody response to GARDASIL 9 was observed for 3 years in girls and boys who were 9 through 14 years of age at time of vaccination receiving 2 doses at 6-month or 12-month interval. At Month 36, non-inferiority criteria were also met for GMTs in girls and boys 9 through 14 years of age receiving 2 doses at a 6-month interval (+/-1 month) compared to GMTs in women 16 through 26 years of age receiving 3 doses of GARDASIL 9.
Duration of protection of a 2-dose schedule of GARDASIL 9 has not been established. (See Table 9.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageVariation in Dosing Regimen in 16-through 26-Year-Old Women: All individuals evaluated for efficacy in the PPE population of Protocol 001 received all 3 vaccinations within a 1-year period, regardless of the interval between doses. An analysis of immune response data suggests that flexibility of ±1 month for Dose 2 (i.e., Month 1 to Month 3 in the vaccination regimen) and flexibility of ±2 months for Dose 3 (i.e., Month 4 to Month 8 in the vaccination regimen) do not substantially impact the immune responses to GARDASIL 9 [see Dosage & Administration - Administration of GARDASIL 9 In Individuals Who Have Been Previously Vaccinated With GARDASIL].
Persistence of Immune Response to GARDASIL 9: The persistence of antibody response following a complete schedule of vaccination with GARDASIL 9 is being studied in a subset of individuals who will be followed up for at least 10 years after vaccination for safety, immunogenicity and effectiveness.
In 9- through 15-year-old boys and girls (Protocol 002), persistence of antibody response has been demonstrated for at least 10 years; depending on HPV type, 81 to 98% of subjects were seropositive.
In 16- through 26-year-old girls and women (Protocol 001), persistence of antibody response has been demonstrated for at least 5 years; depending on HPV type, 78 to 100% of subjects were seropositive. Efficacy was maintained in all subjects regardless of seropositivity status for any vaccine HPV type through the end of the study (up to 67 months postdose 3; median follow-up duration of 43 months).
GMTs for HPV-6, -11, -16 and -18 were numerically comparable in subjects who received GARDASIL or GARDASIL 9 for at least 3.5 years.
Evidence of Anamnestic (Immune Memory) Response: Evidence of an anamnestic response was seen in vaccinated women who were seropositive to relevant HPV type(s) prior to vaccination. In addition, women (n = 150) who received 3 doses of GARDASIL 9 in Protocol 001 and a challenge dose 5 years later, exhibited a rapid and strong anamnestic response that exceeded the anti-HPV GMTs observed 1 month postdose 3.
Administration of GARDASIL 9 to Individuals Previously Vaccinated with GARDASIL: Protocol 006 evaluated the immunogenicity of GARDASIL 9 in 921 girls and women (12 through 26 years of age) who had previously been vaccinated with GARDASIL. Prior to enrollment in the study, over 99% of subjects had received 3 injections of GARDASIL within a one year period. The time interval between the last injection of GARDASIL and the first injection of GARDASIL 9 ranged from approximately 12 to 36 months.
Seropositivity to HPV Types 6, 11, 16, 18, 31, 33, 45, 52, and 58 in the per protocol population ranged from 98.3 to 100% by Month 7 in individuals who received GARDASIL 9. The GMTs to HPV Types 31, 33, 45, 52, and 58 were lower than in the population who had not previously received GARDASIL in Protocols 001, 002, 005, 007 and 009. Efficacy of GARDASIL 9 in preventing infection and disease related to HPV Types 31, 33, 45, 52, and 58 in individuals previously vaccinated with GARDASIL has not been assessed.
Concomitant Use of GARDASIL 9 with Other Vaccines: Menactra [Meningococcal (Groups A, C, Y and W-135) Polysaccharide Diphtheria Toxoid Conjugate Vaccine] and Adacel [Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine Adsorbed (Tdap)]: In Protocol 005, the safety and immunogenicity of co-administration of GARDASIL 9 with Menactra [Meningococcal (Groups A, C, Y and W-135) Polysaccharide Diphtheria Toxoid Conjugate Vaccine] and Adacel [Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis Vaccine Adsorbed (Tdap)] (same visit, injections at separate sites) were evaluated in a study of 1,237 boys and girls 11 through 15 years of age at enrollment.
One group received GARDASIL 9 in one limb and both Menactra and Adacel, as separate injections, in the opposite limb concomitantly on Day 1 (n = 619). The second group received the first dose of GARDASIL 9 on Day 1 in one limb then Menactra and Adacel, as separate injections, at Month 1 in the opposite limb (n = 618). Subjects in both vaccination groups received the second dose of GARDASIL 9 at Month 2 and the third dose at Month 6. Immunogenicity was assessed for all vaccines 1 month post completion of the vaccination series (1 dose for Menactra and Adacel and 3 doses for GARDASIL 9).
Concomitant administration of GARDASIL 9 with Menactra and Adacel did not interfere with the antibody response to any of the vaccine antigens when GARDASIL 9 was given concomitantly with Menactra and Adacel or separately.
Repevax [Diphtheria, Tetanus, Pertussis (acellular, component) and Poliomyelitis (inactivated) Vaccine, (adsorbed, reduced antigen(s) content) (dTap-IPV)]: In Protocol 007, the safety and immunogenicity of co-administration of GARDASIL 9 with Repevax [Diphtheria, Tetanus, Pertussis (acellular, component) and Poliomyelitis (inactivated) Vaccine, (adsorbed, reduced antigen(s) content) (dTap-IPV)] (same visit, injections at separate sites) were evaluated in a study of 1,053 boys and girls 11 through 15 years of age at enrollment.
One group received GARDASIL 9 in one limb and Repevax in the opposite limb concomitantly on Day 1 (n = 525). The second group received the first dose of GARDASIL 9 on Day 1 in one limb then Repevax at Month 1 in the opposite limb (n = 528). Subjects in both vaccination groups received the second dose of GARDASIL 9 at Month 2 and the third dose at Month 6. Immunogenicity was assessed for all vaccines 1 month post completion of the vaccination series (1 dose for Repevax and 3 doses for GARDASIL 9).
Concomitant administration of GARDASIL 9 with Repevax did not interfere with the antibody response to any of the vaccine antigens when GARDASIL 9 was given concomitantly with Repevax or separately.
Serious Adverse Events in Clinical Trials of GARDASIL 9: Serious adverse events were collected throughout the entire study period for the seven integrated clinical studies for GARDASIL 9. Out of the 15,778 individuals who were administered GARDASIL 9 and had safety follow-up, 356 reported a serious adverse event; representing 2.3% of the population. Four individuals administered GARDASIL 9 reported at least one serious adverse event that was determined to be vaccine-related. Four vaccine-related serious adverse events that occurred during the study period were pyrexia, allergy to vaccine, asthmatic crisis and headache.